Year
62 year old woman presented to Emergency department with h/o intermittent headache with associated nausea and vomiting, giddiness, difficulty in walking and imbalance, blurring of vision, for 1 month – No h/o seizures, posturing, altered sensorium. Vomiting increased in episodes for last 2 days; Unable to walk at present. No other co-morbidities. CT Scan – solitary intraventricular cystic lesion 3 cm diameter causing hydrocephalus. Cyst removed in toto due to evidence of ependymal inflammation.
- Diagnosis
- How does man acquire the infection
- What are the differential diagnosis
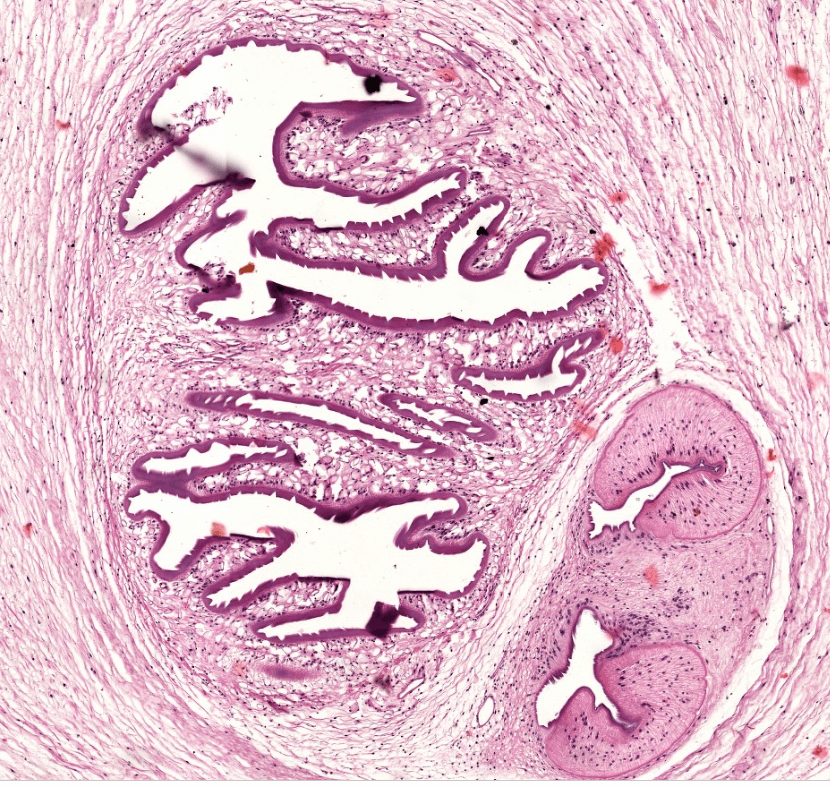
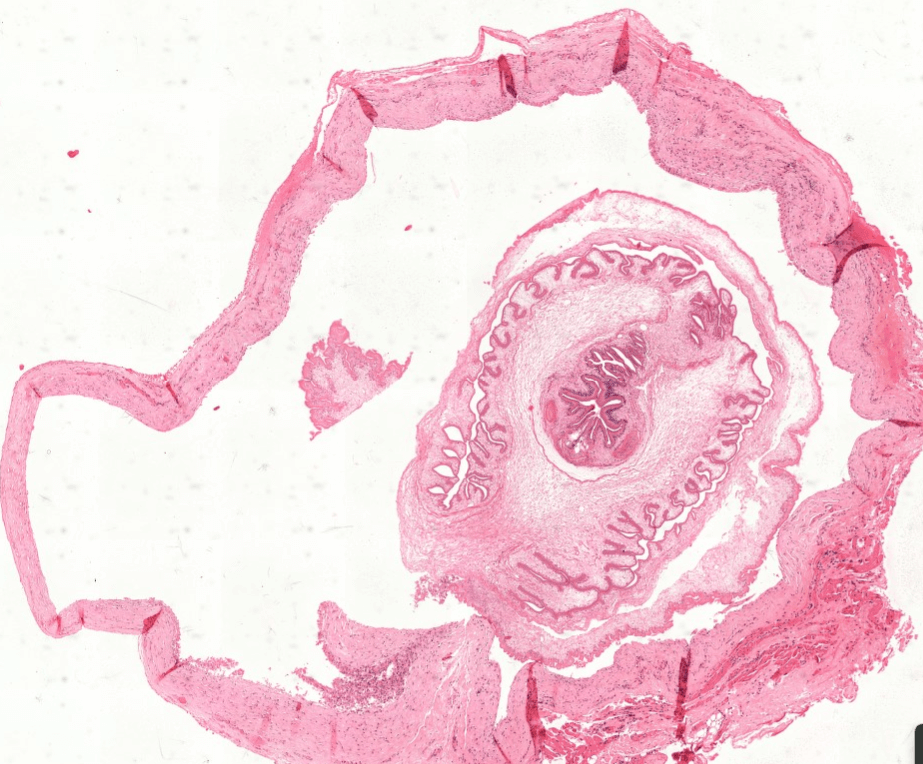
Following images are Histopathological examination of the cystic lesion

Case answer – Posted on: 13-Jan-2024
- Neurocysticercosis- the HPE shows cysticercus cellulosae which are ovoid, opalescent, contain an armed scolex invaginated into a fluid-filled bladder. Common cause of epilepsy in endemic areas (50-80% of cases) – varied symptoms usually caused by degrading or calcification of cyst not “live” cysts including psychiatric symptoms, stroke or spinal cord compression
- Man acquires neurocysticercosis by consumption of eggs of T.solium either by ingestion of contaminated food and water or by autoinfection either due to unhygienic habits or due to reverse peristalsis by which gravid segments throw the eggs into the stomach
- Differential diagnosis- TB, metastasis, abscess, toxoplasmosis, hydatid cyst, glioma